

Guest post: Does a negative wealth shock affect your health?
Evidence from an episode of 'expropriation with partial compensation' in nineteenth-century South Africa


How are wealth and health connected? At a macro scale, a quick inspection of the World Population Prospects database curated by the United Nations shows that people tend to live longer in richer economies. The wealthier, the healthier. But how does that manifest on an individual level? Presumably just earning more money does not make anyone automatically healthier.
The link between wealth and health might operate through several mechanisms. For example, earning more money means access to healthier goods, such as foodstuffs. It also means access to better areas to live in, where air and noise pollution is greatly reduced. In countries without socialized healthcare, the ability to afford good health insurance can be key to living better, longer lives. Yet, this relationship is not necessarily linear. Conditional on an individual’s educational level, consumption patterns may vary considerably. Activities detrimental to health such as drinking and smoking also become proportionately cheaper as one gets wealthier. If wealth levels increase to the point that they lead to early retirement or even voluntary joblessness, one may also need to consider mental health repercussions. There are well-documented effects of positive mental health benefits of having activities that keep the mind stimulated, such as a regular job.
Still, on average, having more wealth leads to a healthier life. But the same data could be interpreted in the opposite direction. Instead of just looking at the relationship through the lens of wealth causing health, we can also think about this relationship as health causing wealth. While it is true that wealth increments enable individuals to access healthier goods, one can postulate that wealth requires health to begin with. Here we can also imagine several mechanisms. Healthier individuals may miss fewer workdays due to sickness, leading to increased productivity and thus, wealth. Some chronic illnesses may limit an individual’s ability to pursue certain careers that are deemed more profitable. Unhealthy childhoods are oftentimes the result of general infrastructure problems such as basic sanitation, which may prevent people from maximizing their earnings potential and keep them trapped in a vicious circle of poverty and, obviously, unhealthy circumstances.
Another layer of complexity pertains to the intergenerational transmission of such effects. If individuals are trapped in an unhealthy setting, their offspring will likely inherit the condition, hindering successive generations. Congenial problems are also likely to be carried through the next generation. Similarly, wealth can be inherited, and thus all the health benefits associated with it.
Now we have a classic endogeneity problem. What comes first? Testing such a relationship is extremely challenging. Randomizing the wealth of people to test its effects on health would be plainly unethical. Under these circumstances, economic history may be able to contribute.
Economists are often interested in ‘natural experiments’, i.e. an event that naturally creates a control and a treatment group. This way, we can test certain hypotheses that would not be feasible in a controlled experiment. This is precisely what our paper, written with Jeanne Cilliers and Johan Fourie and published earlier this year in Explorations in Economic History, does. By using the 1834 emancipation of slaves in the Cape Colony, we test how and to what extent wealth variations can explain health outcomes in the slaveholder population. While this is an event whose social and historical significance for the enslaved populations of the British Empire cannot be overstated, an aspect of particular interest to economic historians is the cash compensation paid to slaveholders.
The records show that former slaveholders received, on average, between 40 and 50% of the value of their slaves. From an economic standpoint, therefore, emancipation represented the loss of wealth or, put differently, the loss of an asset. But there is more: these shortfalls, i.e. the difference between the ‘slave wealth’ and the compensation paid, were random across slaveholders. Randomness arose from the criteria used at the time to determine the compensation. While slaves were appraised using market prices – and many characteristics were, therefore, considered, such as age, place of origin, height, weight, sex, and occupation – compensation was awarded based exclusively on two criteria: sex and the occupation of the enslaved person. In such a scenario, whereby slaves within the same category were considered homogeneous, it is easy to see that the overlay between the appraisal and the compensation process will generate a residual shortfall that is independent of any observable characteristics. It allows us to categorize former slaveholders based on shortfalls in a quasi-experimental setting.
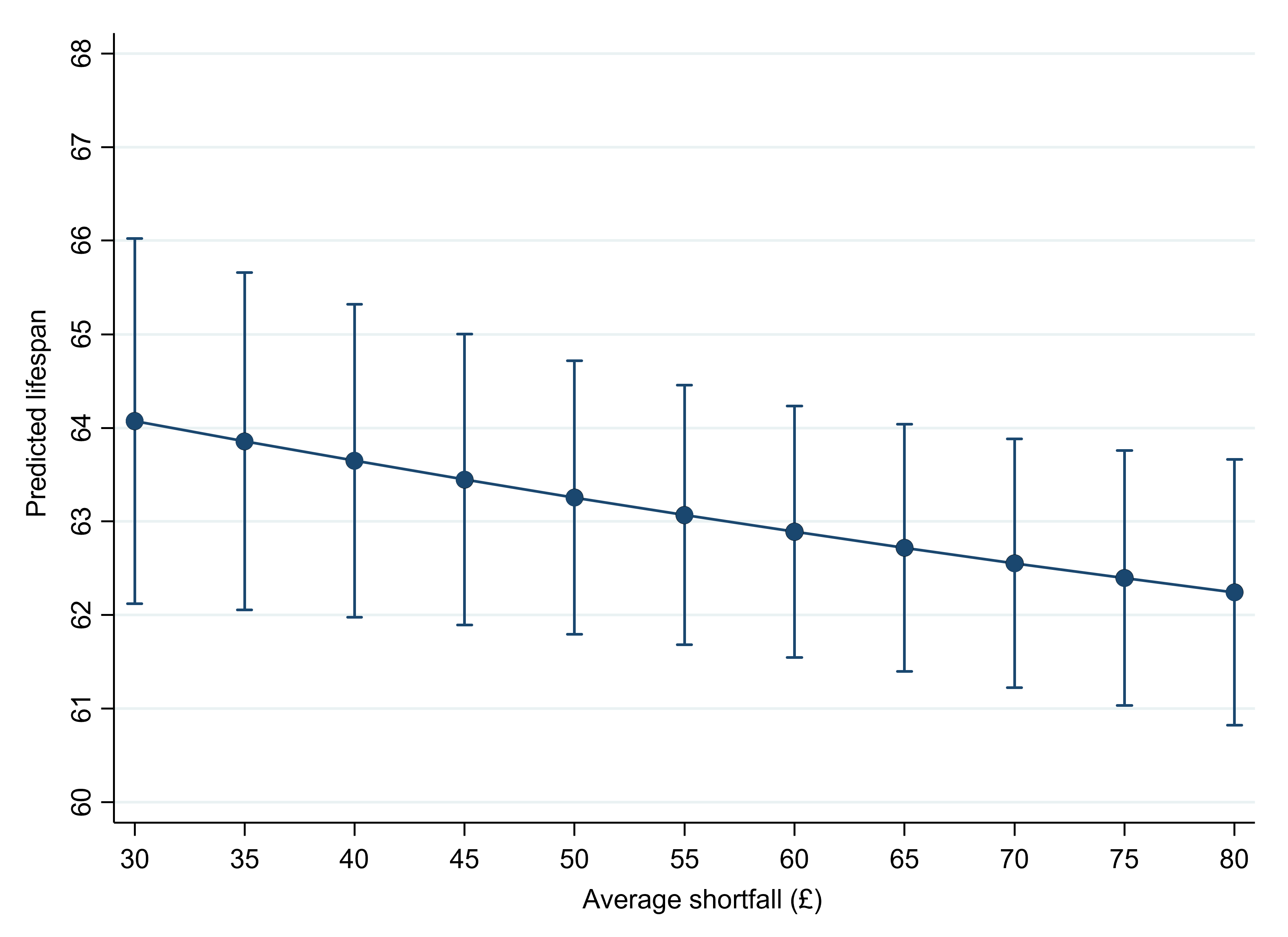
From that point, we were interested in identifying any health-related outcomes produced by these shortfalls. We found the means to do this by linking data from three different datasets containing compensation claims, genealogical records, and tax records. Our results suggest that shortfalls do have an impact on lifespans, but that these effects are usually small and that they are not distributed homogeneously across our population as older cohorts seem to be absorbing most of the estimated negative effects. The relationship between shortfalls and lifespans is given in the figure below, where it is clear that wealth losses have a direct if small effect on lifespan.
Having a research setting such as ours offers many advantages. Firstly, we are not looking at an exogenous wealth gain, but rather at the loss of an asset that was the most important source of wealth for our population of interest. It gives us a unique glimpse into an effect hard to capture in contemporary and other experimental settings. Moreover, the historical setting we use means that individuals had fewer coping mechanisms to deal with wealth losses. Studies of present-day settings find that extensive social security nets reduce the effects of wealth on wealth-mortality gradients. While anecdotal evidence suggests that the population of slaveholders at the Cape were able to rely upon family networks in times of economic duress, this is far from comparable to social security systems in the developed countries of the 21st century.
More importantly, however, these findings are not confined to the population of slaveholders (and their descendants) we studied. Negative wealth shocks, such as expropriation, have detrimental but limited effects on the health of the affected population, even if the wealth shocks are relatively large. We might interpret this, too, as saying that a positive wealth shock for a population above a certain living standard won’t make much of a difference to health. Instead, health outcomes are more likely to be affected by large-scale programs that target infrastructure and create incentives for different behavioral patterns, which tend to be a lot ‘stickier’ and are likely to be transmitted to future generations.
Igor Martins is a postdoctoral fellow at the University of Cambridge (UK) and Lund University (Sweden). The paper, co-authored with Jeanne Cilliers and Johan Fourie, is published in Explorations in Economic History. Photo by Juanita Swart on Unsplash.
 | A guest post by
|